Platelet rich plasma
Preface
Platelet-rich plasma (PRP) is on everyone’s lips. PRP is a part of the human blood that is removed before surgery, processed and then given to the patient. The effects achieved thereby significantly contribute to improved wound healing, tissue regeneration and even about “rejuvenation” is spoken. The application of PRP seems to have no limits. The fact that the interest of both laymen and scientists is unbroken may be illustrated by the following facts: If the global Google trends for PRP are called, the first search results include the requests “prp treatment” (1st place), “prp injection” ( 3rd place) and “prp therapy” (4th place). Places 2 and 5 are occupied by “prp hair” or “prp hair treatment”. The following graph shows, how the popularity of Google searches for the term PRP in recent years increased.
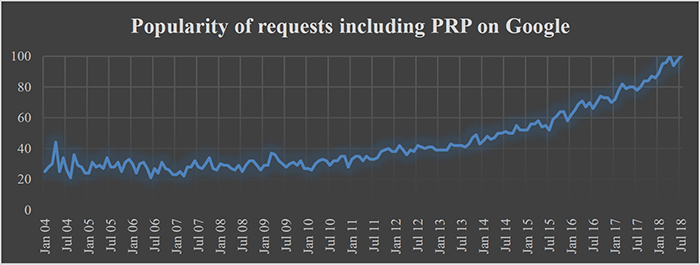
Figure 1: PRP as a search term in Google search
But not only in the general searches on Google, there is an enormous interest in PRP. A similar effect can be observed when the large scientific-medical database PubMed is searched for PRP. The following chart shows the studies and articles published each year about PRP.
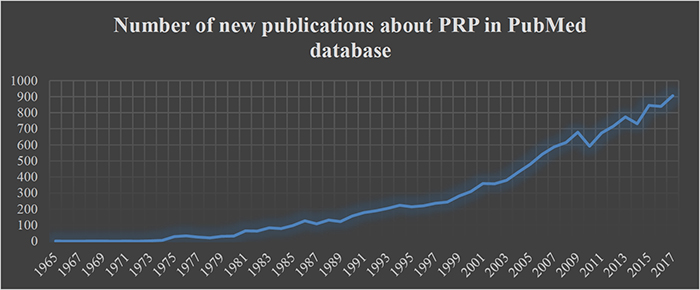
Figure 2: Number of new publications about PRP in PubMed database
But how is this tremendous interest in PRP explained and why does it seem to play a special role as a treatment approach for hair loss in particular?
Basically, PRP is suitable for an almost intangible number of medical applications or is currently being investigated for its suitability. In my new article, however, I would like to explain why it seems to play a special role, especially in connection with the treatment of various forms of hair loss and why it is doubtful that PRP represents a suitable treatment approach for all hair loss problems. In addition, I give you additional background information about PRP and its possible applications. With this information, you should ultimately be able to judge for yourself whether PRP can be a useful treatment approach for hair loss in your eyes or not.
Therefore, enjoy reading!
Sincerely
Yours, Angela Lehmann
Platelet-rich plasma as a treatment for hair loss
Platelet-rich plasma (PRP) has become of great therapeutic importance for many medical procedures and applications. This is a specific part of the blood serum in which the platelets were enriched by centrifugation. PRP is also being promoted by some providers with the promise that it is a reliable treatment for hair loss. So in my new article, I would like to introduce you to what PRP is, what it does and what its therapeutic value may be in different forms of hair loss.
PRP – History, Production and Application
Basically, PRP is human blood plasma (mainly the blood without the red blood cell erythrocytes), which is enriched with another type of blood cell called platelets. Original PRP is always autologous, which means that the person treated with the PRP is always the donor from whose blood PRP was made. As a result, there are no rejection reactions when treated with PRP. In addition, PRP can be easily obtained from a blood donor by centrifugation so that its production is very favorable compared to many other medical procedures.
The history of the use of PRP goes back to the 1970s, when researchers began to experiment with blood components to produce tissue-like materials for surgery. An important milestone in this context was the development of fibrin glue in the 1970s. Fibrin is simply the glue that “hardens” when blood clotting is activated. At that time, the researchers succeeded in the fact that the fibrin cross-linked by the addition of thrombin (protein) and calcium outside its physiological environment and so “hardened”. As a result, they had produced the first biocompatible adhesive. This adhesive was further developed into fibrin gel in the 1990s, which was able to withstand the normal pressures of blood flow in vessel walls and was also very similar to human tissue in terms of its mechanical properties. In subsequent experiments, platelets were added to the fibrin gel, as it was found that the platelets obviously have a positive effect on the healing with fibrin-glued pieces of tissue. This additional use of platelets may be considered as the first time use of PRP.
As already mentioned, the production of PRP is a simple, fast as well as inexpensive process. Basically, the surgeon or therapist only needs one centrifuge, which is part of the standard equipment in each laboratory. The manufacturing process begins with taking a defined amount of blood from the patient’s arm vein. This is collected in a tube called monovette and centrifuged directly.
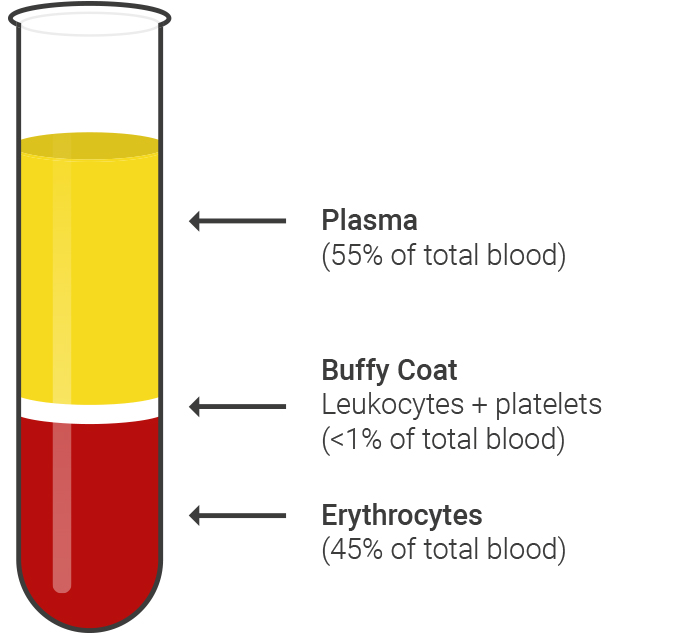
Figure 3: Schematic representation of the first centrifugation step
After an initial centrifugation step, several basic blood components have separated from each other, as the figure above illustrates schematically:
In the lower part of the Monovette volume accounting for about 45% of the total volume are separated red blood cells (erythrocytes). The blood plasma, in which all the soluble blood components and most platelets are located, makes up the upper part of the Monovette volume and between both parts there is a white trend layer consisting of immune cells (leucocytes) and few platelets. Subsequently, the upper phase with the blood plasma as carefully and completely removed, without touching the buffy coat layer, and transferred to a new tube. There is a second centrifugation step, which serves to enrich the platelets at the bottom of the tube. The supernatant plasma can then be removed again and the platelets located on the tube bottom can be resolved in any amount of plasma, so that the practitioner can adjust the concentration of the PRP.
As mentioned at the beginning of the article, there are many applications for PRP in surgery today and in medicine in general. Treatment focuses are in particular bone fractures, tendonitis, poorly healing wounds or such wounds, in which a large-area scar formation is to be expected, which should be avoided as possible, a slow bone regeneration, such as osteoporotic patients, or joint diseases. In addition, applications such as wrinkles, erectile dysfunction or hair loss are being researched. The possible fields of application of PRP are extremely versatile. But how is this explained? In order to get closer to the answer to this question, the following is more specific about the (probable) mechanism of action of PRP.
How does PRP work?
At this point, it is important to first of all talk about a “probable” mechanism of action, since the bioactive molecules contained in the PRP are so numerous and so diverse that probably not one single pathway can be identified, but the actual effect of the PRP is probably based on the interaction of the individual components. How exactly this interaction of the individual factors and molecules is, however, is the subject of current research and can therefore not be explained in more detail here.
So far, numerous scientific publications have attempted to elucidate the mode of action of the PRP components, and important findings could also be compiled. Although these can not be discussed in detail, Alsousou, Thompson, Hulley, Noble and Willett (2009), for example, offer a good overview here. Nonetheless, an attempt will be made below to explain the mechanism of action in an understandable and simple manner:
When a person cuts his or her finger during kitchen work, many physiological and biochemical processes occur simultaneously, so that such a minor injury does not endanger one’s life. Initially, blood clotting sets in, causing the escaping blood to solidify and seal the wound. If that did not happen, very large amounts of blood could be lost even over the smallest of injuries. The injured cell boundaries cause the contents of the skin cells to leak out and enter the injury zone, alerting immune cells in the vicinity of the injury, which migrate to the site of the injury and trigger an inflammatory reaction there. This usually happens through bioactive proteins and other signaling substances. These result, for example, in a slight swelling of the wound, as lymphatic fluid accumulates around the wound with other immune cells and the tissue around the lesion becomes red. This immune response is initiated by the body to help prevent any pathogens that may have invaded and “dispose of” the damaged and non-viable skin cells.
These processes are all performed and controlled by highly specialized body and blood cells by means of various biochemical and physiological stimuli. However, at this stage only the “damage done” has been eliminated. The reconstruction of the tissue injured by the incision (i.e. the actual regeneration) takes place in a second step and is partly controlled by other cell types. For example, the immune cells must leave the former wound site, the tissue swelling must decrease, and some cells may need to repair damaged blood vessels; in the case of more severe injuries, bone substance may need to be re-formed and much more. And that’s exactly what PRP‘s mechanism of action is all about: By administering PRP to injured tissue (for example, in the course of an operation), the healing and regeneration of the tissue is accelerated by the fact that the platelets in the PRP represented the entire signal sequence that the body “naturally”, slowly and by no means so strongly in the form of released biomolecules (these are mainly growth factors). It is, so to speak, a “boost” for normal wound healing. However, it is important to anticipate Chapter 3 of this article, because hair loss is not usually a “injury” like what happens in a bicycle accident or the inadvertent handling of kitchen knives.
At this point, however, it must again be pointed out that the biological effects and effects emanating from the mixture of growth factors are so diverse that they can not be assigned to a single constituent. This makes it almost impossible to answer the question of why and how exactly PRP affects the individual patient.
Why the effects of PRP on hair loss should be considered critically
Right from the start, it must be made clear that PRP is by no means suitable as a hair-growing agent, but has many positive effects in other medical applications. In many cases where there is a medical indication, PRP has been shown to provide extremely good effects on tissue regeneration, healing of dental or hip implants, or scar prevention, but it is doubtful that such results could be achieved for the treatment of hair loss. But why is that?
First of all, it has to be said that the most common form of hair loss, androgenetic alopecia, is not an injury of physiologically intact skin. Rather, this form of hair loss based on the fact that degradation products of the male sex hormone testosterone unfold a toxic effect on the hair follicles and these die as a result. However, these are “normal” physiological processes in which the PRP can not support: Regeneration of the tissue as after a fracture or a cut injury is not necessary and therefore PRP does not help.
Furthermore, it must also be noted that it is a qualitative difference whether the regeneration of skin tissue can be supported so that virtually no scars remain or the healing time is significantly shortened or whether it comes to the formation of a new complete organ, as it would be necessary in the case of androgenetic alopecia. It should be noted here that a hair follicle is nothing more than a highly complex and specialized organ of the human body that performs a specific task.
It can also be stated that a large number of studies dealing with the effects of PRP treatment on hair growth do not treat androgenetic alopecia, but rather a form of hair loss called alopecia areata (Trink et al., 2013). This is the so-called circular hair loss that usually occurs in the second and third decade of life without a recognizable cause and can represent a reversible form of hair loss. The crucial difference to androgenetic alopecia, however, is that the hair follicles are preserved and viable in the case of alopecia areata, so that application of PRP may well be associated with positive effects, without today, as mentioned above, knowing the exact mechanism of action. So, if the users of PRP for hair loss with the predicates become “clinically tested” or “clinical studies”, those interested should always be aware of what type of hair loss was actually treated in the study.
As mentioned in my earlier article (The Relevance of Clinical Trials for the Treatment of Hair Loss), people who are interested in treating hair loss should always inform themselves about exactly what they have to do with it in the end when looking for clinically tested products and methods, because often this predicate is not the expression of high scientific quality, but only advertising messages. In the case of PRP, whose effectiveness in hair loss is allegedly clinically proven, you can also orientate yourself to the following questions:
- Has any study been published and, if so, in which journal?
- How were the findings generated in the study?
- Have any side effects been reported, is there an indication of manageability, or does the effect have a limited duration, so the application must be retrieved?
- Are inadmissible generalizations drawn from the results of the study or is there a transfer of knowledge about different “diseases” (androgenetic alopecia versus alopecia areata)?
- Are there any methodological or financial ambiguities regarding the published data? For example, does a company that may be co-financing the study deal with the production of products designed to facilitate the use or production of PRP or do authors of the study receive donations from such companies?
In this context, I would also like to ask you, in the case of hair loss treatment via PRP, to be vigilant and not to recklessly put your trust in any providers and their advertising messages. If you have any questions concerning the use of PRP or hair loss treatment in general, I would like to invite you to arrange a personal consultation with us at our clinic.
Sincerely
Yours, Angela Lehmann
References
Alsousou, J., Thompson, M., Hulley, P., Noble, A. & Willett, K. (2009). The biology of platelet-rich plasma and its application in trauma and orthopaedic surgery: a review of the literature. The Journal of bone and joint surgery. British volume, 91(8), 987–996.
Marx, R. E. (2004). Platelet-rich plasma: evidence to support its use. Journal of oral and maxillofacial surgery, 62(4), 489–496.
Trink, A., Sorbellini, E., Bezzola, P., Rodella, L., Rezzani, R., Ramot, Y. & Rinaldi, F. (2013). A randomized, double‐blind, placebo‐and active‐controlled, half‐head study to evaluate the effects of platelet‐rich plasma on alopecia areata. British Journal of Dermatology, 169(3), 690–694.