Bodyhair – the next revolution ?
Preface
Dear readers,
While in the wild many species of mammals protect themselves with a dense coat against strong temperature fluctuations and harmful UV radiation, or this is also important for camouflage, such necessities in humans usually no longer exist. It is therefore assumed that humans lost their coat in the course of evolution, because of having dwellings, clothes or his role as a hunter. Hence, there was no more need for a thick coat. Nonetheless, human hair can be found in more body regions than just the head. Depending on age, gender and ethnic origin, there is more or less pronounced hair in the face (as a beard), in the axillary region, in the pubic area as well as on the chest. Depending on the ethnic origin, the arms, legs and back may also be hairy. Such hair is also referred to as a body hair.
Due to the fact that some people who want to undergo a hair transplantation have no sufficiently large donor area on the head, it was considered relatively early to transplant the hair (or more precisely, the hair follicles) of other body regions to the scalp and so possibly recover hair lost or thinned out as a result of alopecia. Such an idea was first theoretically described in 1939 by Okuda. However, it should take until the year 2001 when such a transplantation was successfully carried out first. Over time, the body hair transplantation has also established itself in the market economy, so that there are now a large number of providers who offer body hair transplantations.
However, there are several questions: What exactly is behind the promise of these providers to be able to transplant body hair on the head? Can body hair be used to achieve an aesthetically equivalent treatment result compared to transplanting hair from the head? I would like to answer these and other questions about body hair transplantation in my new article.
Therefore, enjoy reading!
Sincerely Yours,
Angela Lehmann
Body Hair Transplantation – a Revolution in Hair Transplantation?
The idea of transplanting hair from all regions of the body (body hair) to the scalp, if the donor area is insufficient in the case of a planned hair transplant, was first published in 1939. At least since the turn of the millennium, such interventions are possible. But do they actually constitute a meaningful medical intervention? Why I am skeptical about body hair transplantation and would not recommend it, I described to you in my new article about body hair transplantation.
Why does the transplantation of body hair seems to be interesting for the hair transplantation?
Basically, in the course of a hair transplantation follicles grafted from one point of the body (donor area) are transplanted to another (recipient area). Strictly speaking, it is not the hair that is transplanted, but the hair follicles from which the hair grows. Mainly, such treatment is interesting for people who suffer irreversible hair loss. This can be the case, for example, as a result of an accident or illness (androgenetic alopecia). Hair follicles are then removed from the back of the head and transplanted to the hairless areas.
This method of autogenous hair transplantation, however, has natural limits because humans have only a limited number of hair follicles on the head and for aesthetic and medical reasons, not all hair follicles are available for transplantation. Thus, in the case of a European, follicles of 17 to 18 square centimeters of scalp donor area can be removed and transplanted during a hair transplant session. This corresponds to approximately 3,400 to 3,600 hair follicles. In the case of an optimal donor area, this procedure may be repeated up to four times, as long as there is a medical-aesthetic need for it. It follows that theoretically a maximum of 15,000 hair follicles can be transplanted during an autogenous hair transplantation, but some patients desire or even need to transplant more than this natural maximum to achieve an aesthetically pleasing treatment result.
For this reason, as early as the end of the 1930s, the first consideration has been made whether it could also be possible to transplant hair follicles from other body parts on the head. These considerations particularly concerned hair follicles of the scalp, eyebrows, armpits and pubic area for restoring hair in cases of alopecia on the head and pubic area. However, it took until the year 2001 when the first successful transplantation of body hair was made. Small injection needles were used to extract individual follicles from the facial skin. The extracted follicles were used to reconstruct the eyebrows of patients. The authors themselves describe their outcome as very positive and the procedure would not have been associated with scarring. Furthermore, the removal of the follicles is called an elegant, fast and less invasive method of obtaining body hair follicles for transplantation.
What properties does body hair have?
However, as will be shown in the following section, hair is not the same as hair. This difference is due to the fact that the hair of different body regions also have different properties. These differences will be discussed below.
Most of the hair of the human body can be assigned to the so-called Vellus hair. Vellus hairs are fluffy and have no medulla within the hair shaft. For this reason, they have an extremely fine structure and are basically not suitable for a body hair transplantation. In contrast, hairs of the beard, the trunk, the armpit and the pubic region are basically suitable for a body hair transplantation after they have matured into terminal hair during puberty.
An important difference between scalp hair and the hair of other body regions is that the latter hairs go through the hair growth cycle at a different rate than the hair on the scalp. The hair growth cycle starts in the anagen phase (growth phase), in which a new hair root is formed in the follicle and the production of a new hair begins. This is followed by the catagen phase (transitional phase), at the end of which the hair stunted and is lost. The hair follicle now goes into telogen phase (resting phase), which represents a regeneration phase of the follicle. Then the cycle starts again. The body hair follicles are in contrast to scalp hair by a share of 30 to 85 naturally in the telogen phase, in which no hair shaft is produced. In contrast, between 85 and 90 percent of scalp hair is normally in the anagen phase, forming a hair shaft. It should also be noted that the body hairs undergo a much shorter (a few months) anagen phase than hair on the head, where the anagen phase usually lasts several years. In the case of a body hair transplantation to the scalp, it must be remembered that the transplanted hairs go faster through the hair cycle and produce fewer hair shafts, which can significantly influence the aesthetic treatment result. Because of this altered growth cycle, body hairs are on average also thinner and shorter than scalp hair. Usually only the beard and chest hair are thicker than the hair on the scalp.
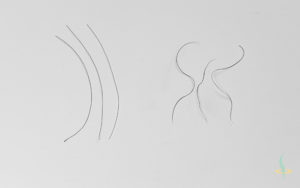
The illustration shows the different texture of scalp (left) and chest hair (right). Especially with regard to the curliness, big differences can be seen.
Furthermore, the scalp hair and the body hair differ in terms of their texture. While the hair on the head may have all textures from completely smooth to heavily curled, the body hair is usually wavy to curled. In many cases, this necessitates adaptation of the hair texture by means of a special care or smoothing of the hair in order to make the grafted body hair the scalp hair more similar and, for example, to prevent the formation of a streak after the transplantation.
Furthermore, the hair follicles of the body hair lay higher up in the skin than it is the case with hair on the scalp. While the follicles of the body hair are located in the epidermis, the hair follicles of the scalp are anchored in the subcutaneous tissue. In addition, body hair occurs at a more acute angle from the skin than hair on the head. Especially the latter aspect is important in the course of a body hair transplantation, since the later appearance can be significantly influenced by the angles of the hair shaft. In our clinic this fact is used in the classic scalp hair transplantation by means of the Crosspunch technique developed by me, as by a precise adjustment of the insertion angle of the grafts lead later to a visually higher hair volume.
Another important feature that distinguishes the body hair from the main hair is the density at which the hair follicles appear in a particular section of the skin. While body hair grows almost exclusively from individual hair follicles, the hair follicles on the head occur in follicular units of four to six follicles. The density of the hair follicles is correspondingly much lower in the case of the body hair compared to the hair of the scalp. This circumstance makes it necessary to take follicles from a much larger donor area during a body hair transplantation.
What disadvantages does a body hair transplantation have in comparison to scalp hair transplantation?
A bodyhair transplantation has numerous disadvantages compared to the transplantation of follicles taken from the head, which are already important in prior to the actual surgery. So it must be planned before the operation, which hair of which body regions should be used for a transplantation. Special attention must be paid to the aspects of hair diameter, color, hair texture, growth behavior and the exit angle of the hair shaft. This is associated with a planning effort which should not be underestimated, and which will be increased if the recommendations of some researchers are taken into account, according to which the hairs of different body regions should be transplanted together in order to achieve an optimal treatment result.
Another aspect that urgently needs to be considered is the different proportions of hair follicles during the different growth phases of the hair cycle and the fact that hair from different parts of the body goes through this cycle at different speeds. For this reason, some people recommend the use of minoxidil, as it is intended to help them reach a synchronisation of the hair growth cycle for hair follicle removal. It is a substance that some physicians use to treat androgenetic hair loss. However, care should be taken in such a treatment that the drug slows further hair loss at best; however, it can not stimulate new hair growth at the sites that have already become bald due to the progressive alopecia. Another disadvantage that must be mentioned is that Minoxidil must then be taken for the rest of life to prevent further hair loss. In addition, minoxidil – like any other drug too – my have numerous side effects. These include headache, itching, redness and high blood pressure as well as increased hair loss, which is why I generally recommend patients to critically consider treatment with Minoxidil.
Like a scalp hair transplantation the transplantation of body hair is a medical procedure, which is associated with certain treatment risks. These are, however, other risks than they would occur in a scalp hair transplantation. This is due to the fact that an invasive procedure in different parts of the body is associated with different risks than the sole removal and transplantation into the scalp. For example, in the course of a body hair transplantation hypopigmentation of the donor areas may occur. The term hypopigmentation refers to a different density of melanin, which is responsible for the natural skin color. Damage to the melanin-producing cells as a result of the removal of body hair would result in less melanin being deposited in the skin, making the affected skin region appear lighter after surgery than the surrounding tissue. Depending on the donor region, this circumstance may represent a severe aesthetic defect and cause further suffering to those affected.
In addition, it can lead to the formation of a so-called keloid. This refers to a benign tumor that is a result of a disturbed skin healing process. It is a proliferation of unspecialized cells of the skin, which is clearly above the normal skin level. Insofar as a keloid is recognized as such and remains under medical observation, this poses no serious health threat, however, the keloid may affect a patient more or less aesthetically, for example, when it occurs on the face. In most cases, the onset of a keloid is associated with a previous injury or surgery and is more likely to occur in certain areas of the body than in others. Particularly prone to keloids is the chest area, especially around the sternum. This is particularly important for the removal of breast hair for the body hair transplantation, since the emergence of a keloid by the practitioner is hard to prevent. There are currently no generalized drug therapies available for the treatment of a keloid and locally only the injection of corticosteroids can be used. However, these in turn are associated with a variety of potentially serious side effects. Surgical removal of the keloid is also not longer practiced nowadays, as reoccurrence of a keloid at the same site previously affected is very likely.
Another class of side effects that a body hair transplantation may have is the occurrence of folliculitis. This term refers to a variety of inflammatory diseases of the hair follicles, which can occur, for example, when it comes to skin irritation, because possibly a transplanted hair continues to grow under the skin instead of exiting the skin. For example, mild forms of folliculitis occur as a so-called barber’s itch. However, there are also more severe forms in which the inflammation so wide spread, that it comes to an infection of the affected skin areas, which must then be treated according to individual aspects with special medication and it can be associated with scarring. The possibly increased occurrence of folliculitis can be explained in the transplantation of body hair by the fact that the transplanted follicles in the case of the body hair are anchored at a different depth in the skin than the hair of the scalp.
In particular, while follicle removal from the face of the therapist must take special care, as in the case of improperly performed surgery there is a risk that the facial nerves are injured. In the worst case, this can lead to a permanent facial paralysis, i.e. (partial) paralysis of the facial muscles. The potential consequences of facial nerve paralysis may include limited facial expressiveness, difficulties closing the eyelids, speech, and eating. In this way, it can lead to a serious restriction of the general health-associated quality of life, which can put the affected to a high level of suffering.
However, probably the most important reason for refraining from a body hair transplantation is that body hair is simply not similar enough to scalp hair due to the reasons mentioned in chapter 2 of this article. The differences in growth behavior, hair diameter, thickness and color are too serious to achieve a treatment result comparable to classic hair transplantation. This also applies if the hair follicles of various body regions have been transplanted to the head in combination, as recommended by some physicians. In addition, the planning effort for such an intervention would be so immense that, realistically, it would hardly be possible to cope with it. Even if a patient would be willing to accept that with a body hair transplantation no comparable treatment result as with a scalp hair transplantation could be achieved, there is a risk due to the mentioned side effects and it is highly questionable whether taking these risks justifies the actual treatment goal.
At least as far as the aesthetic aspects are concerned, some dubious providers of body hair transplantation advertise that the grafted hairs would adapt in appearance and texture to the hair of the head after treatment in some unspecified way. However, several arguments can be countered: In the nearly 100 years that the physicians now perform hair transplantation, it has never been observed that once transplanted hair follicles produce different hair shafts than they did before transplantation. So there is simply a lack of empirical proof that such information can be transferred. Furthermore, it should be noted that today no biochemical or physiological process is known by which such information transfer should be possible. In addition to the facts so that never before such a change was observed, it could not be meaningfully explained, if it occurred. And third, it must also be taken into account that if there was an adaptation to the scalp hair in terms of texture and color, then the transplanted body hair in the head area affected by alopecia would also have been lost quickly, as it would also increase sensitivity to alopecia-causative factors, such as the metabolic products of testosterone.
For these reasons, I am very critical about a body hair transplantation, and if you are potentially interested in a hair transplantation, I would also urge you to take a skeptical attitude. In any case, seek in-depth, intense and personal counseling from a potential therapist and make clear the potential risks of treatment, so that you can make a rational and informed decision about whether you are willing to take those risks for the benefit to achieve the desired goal. If you are interested in a hair transplant, I would like to encourage you to contact me to arrange a personal consultation in our clinic.
References
Hirai, T., Inoue, N. & Nagamoto, K. (2001). Potential use of beards for single-follicle micrografts: convenient follicle-harvesting technique using an injection needle. Annals of plastic surgery, 47(1), 37–40.
Okuda, S. (1939). Clinical and experimental studies of transplantation of living hairs. Jpn J Dermatol Urol, 46, 1–11.
Saxena, K. & Savant, S. S. (2017). Body to scalp: Evolving trends in body hair transplantation. Indian dermatology online journal, 8(3), 167.